

E-newsletters
Mar 2024: Spotlight on Women’s Wellness: The Impact of POCUS in Breast Health

In celebration of Women’s History Month, this newsletter edition focuses on the pivotal role of ultrasound in breast health. Recognizing the importance of early detection in combating breast cancer, ultrasound serves as a crucial adjunct to mammography, especially for women with dense breast tissue. By enhancing sensitivity and facilitating lesion characterization, ultrasound significantly improves diagnostic accuracy and patient outcomes. Let’s continue to champion education, early detection, and ultrasound innovation, empowering women to take control of their health journey.
As healthcare professionals, we recognize the critical role of early detection in combating breast cancer, the most common cancer in the world, with half of women diagnosed before the age of 62. According to the United States Preventive Services Task Force (USPSTF), in the US breast cancer accounts for about 30% of all new cancer cases, and black women are 40% more likely to die from breast cancer and are diagnosed at younger ages. Additionally, 5-10% of cancers can be linked to known gene mutations with BRCA 1 (up to 72% lifetime risk) and BRCA 2 (up to 69% lifetime risk) genes being the most common.
The US Preventive Services Task Force emphasizes the importance of mammography screening for women aged 50 to 74, recommending biennial screening. For women aged 40 to 49, the decision to begin biennial screening should be an individual one, considering the patient’s values, preferences, and health history. Mammograms utilize The Breast Imaging Reporting and Data System (BI-RADS) classification which ranges from 0 (Incomplete: Need Additional Imaging Evaluation) to 6 (Known Biopsy-Proven Malignancy), helping to classify a patient’s risk of breast cancer and recommend appropriate follow-up actions.

While the USPSTF does not specifically recommend routine ultrasound screening for breast cancer, it is often used as an adjunctive tool, especially in women with dense breast tissue where mammography’s sensitivity may be reduced. The sensitivity for breast cancer detection using both mammography and ultrasound increases to 97.3% (Berg 2020).
Common indications of breast ultrasound include (Mendelson 2019):
-
Palpable lump during clinical breast evaluation
-
Axillary lymphadenopathy present on mammogram imaging
-
Women younger than 40 years with certain anomalies
-
Pregnant or lactating women
-
Suspicious abnormality identified on mammogram imaging
-
Nipple discharge
-
Skin retraction or inversion of the nipple
-
Surgical scarring evident on mammogram imaging
-
Gynecomastia
-
Suspicion of ruptured breast implants used to differentiate between intra- and extracapsular ruptures
-
Needle-guided percutaneous breast biopsy
-
Follow-up of patients receiving neoadjuvant chemotherapy
When performing breast ultrasound, describe the lesion using the following features (Malherbe 2024):
-
Shape: Oval, round or irregular
-
Position: Describe relative to a clock face
-
Orientation: Parallel or not parallel
-
Margin: Circumscribed or not, further characterized as indistinct, angular, microlobulated, or spiculated
-
Echo pattern: Anechoic, hyperechoic, complex cystic and solid, hypoechoic, isoechoic, heterogenous
Posterior features: No posterior features, posterior acoustic enhancement, posterior acoustic shadowing, or combined pattern
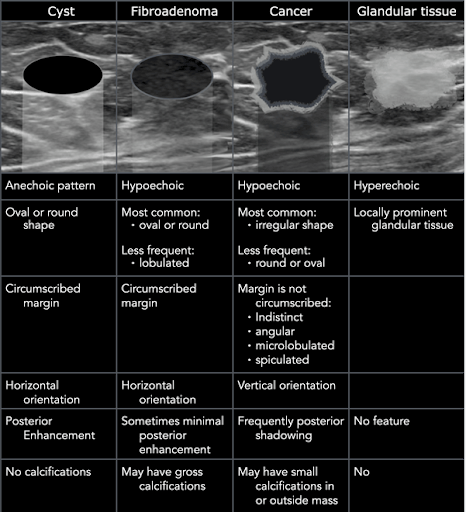
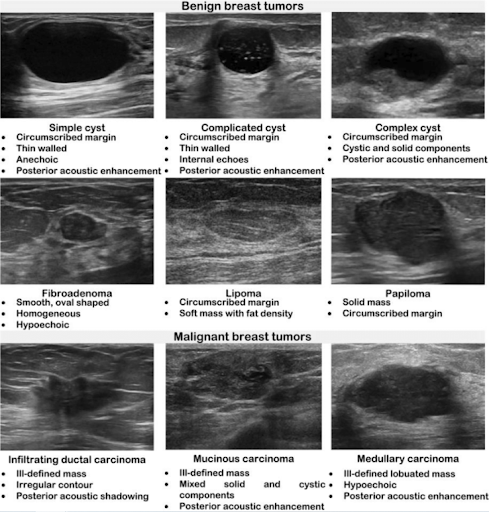
Most common benign morphologic features (Flory 2020):
-
Smooth and well-circumscribed margins
-
Hyperechoic, isoechoic, or mildly hypoechoic in echogenicity
-
Thin echogenic capsule or well-defined capsule border
-
Ellipsoid shape, wider than tall appearance
-
Macrolobulated; <3 lobulated margins
-
Posterior acoustic enhancement
Most common malignant morphologic features (Flory 2020, Vincent 2020):
-
Hypoechoic mass, on occasionally hyperechoic in appearance
-
Spiculated margins
-
Ill-defined borders, architectural distortion of surrounding soft tissue
-
Posterior acoustic shadowing
-
Taller than wide appearance
-
Presence of microcalcifications
As we celebrate Women’s History Month and the significant strides made in breast health, let’s remain steadfast in our dedication to advocacy and innovation. By prioritizing education and early detection strategies, we empower women to take charge of their health journey. Let’s continue to drive progress in breast imaging, ensuring that every woman receives the care and support she deserves. Together, we can make a lasting impact on women’s wellness for generations to come.
—
Resources
- https://www.
uspreventiveservicestaskforce. org/uspstf/recommendation/ breast-cancer-screening. Accessed 02/28/2024. - American College of Radiology. “Breast Imaging Reporting and Data System (BI-RADS).” ACR; https://www.acr.org/Clinical-
Resources/Reporting-and-Data- Systems/Bi-Rads. Accessed 02/28/2024. - Berg WA. Reducing Unnecessary Biopsy and Follow-up of Benign Cystic Breast Lesions. Radiology. 2020 Apr;295(1):52-53. doi: 10.1148/radiol.2020200037. Epub 2020 Feb 18. PMID: 32073379; PMCID: PMC7104697.
- Malherbe K, Tafti D. Breast Ultrasound. [Updated 2024 Jan 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/
books/NBK557837/# - Flory V, Lévy G, Viotti J, Schiappa R, Elkind L, Ghez C, Pellegrin A, Occelli A, Dejode M, Delpech Y, Fouché Y, Figl A, Machiavello JC, Haudebourg J, Peyrottes I, Chapellier C, Barranger E. [Preoperative breast imaging review: Interests and limits of specialized validation in oncology]. Bull Cancer. 2020 Mar;107(3):295-307.
- Vincent-Salomon A, Bataillon G, Djerroudi L. [Hereditary breast carcinomas pathologist’s perspective]. Ann Pathol. 2020 Apr;40(2):78-84
- Kriti, Dr & Virmani, Jitendra & Agarwal, Ravinder. (2020). Deep feature extraction and classification of breast ultrasound images. Multimedia Tools and Applications. 79. 10.1007/s11042-020-09337-z.
- Catalano O, Fusco R, De Muzio F, Simonetti I, Palumbo P, Bruno F, Borgheresi A, Agostini A, Gabelloni M, Varelli C, Barile A, Giovagnoni A, Gandolfo N, Miele V, Granata V. Recent Advances in Ultrasound Breast Imaging: From Industry to Clinical Practice. Diagnostics (Basel). 2023 Mar 4;13(5):980. doi: 10.3390/diagnostics13050980. PMID: 36900124; PMCID: PMC10000574.

History of Present Illness:
A 28-year-old female with a past medical history of bilateral breast mammoplasty and obesity presents to the Emergency Department with acute onset right breast tenderness, erythema, and edema. She also noted a low-grade fever of 38.5 degrees Celsius accompanying these symptoms. The patient underwent bilateral breast mammoplasty 12 months ago and reported a previous episode, approximately 9 months post-surgery, of a small right breast lesion causing discomfort. This lesion fluctuated in size but resolved without intervention. This time, however, the symptoms were more pronounced, with prominent tenderness, warmth, and redness. There were no overlying skin changes, nipple discharge, or recent trauma to correlate.
Physical Examination of Right Breast:
-
Tenderness: Prominent tenderness on palpation around the developing abscess at 2 o’clock with associated palpable fluctuance.
-
Erythema and Edema: Observable redness and swelling on the outer quadrant mentioned above.
-
Calor (Warmth): Increased warmth over the affected breast area.
-
Rubor (Redness): Noticeable redness around the involved area.
-
No Nipple Discharge: No spontaneous nipple discharge.
-
No Overlying Skin Changes: Absence of skin changes over the right breast.

Management:
An ultrasound-guided needle aspiration successfully drained 20 mL of sanguinopurulent material, which was sent for culture. The patient experienced immediate relief and was discharged home with a prescription for a 10-day course of oral amoxicillin-clavulanate (875-125 mg). She received a recommendation for close follow-up with her plastic surgeon for further interventions.
Microbiological Findings:
The initial Gram stain revealed Gram-positive rods, and 5 days later, laboratory data yielded pansensitive growth of Cutibacterium (Propionibacterium) avidum. The patient completed the antibiotic course and scheduled ambulatorial surgical intervention of an epidermoid cyst.
Educational Spotlight:
Pathophysiology:
Postoperative breast abscesses can occur following breast surgery, including mammoplasty. They are often associated with bacteria introduced during surgery, leading to localized infection and abscess formation. The risk factors include obesity, previous surgery, and compromised immune status.
Microbiology:
Cutibacterium (Propionibacterium) avidum is a Gram-positive anaerobic bacterium typically found on human skin. While considered part of the normal skin flora, it can cause infections, especially in the context of surgical procedures. It is crucial to identify the causative microorganism to guide appropriate antibiotic therapy.
Antibiotic Management:
The choice of antibiotics for postoperative breast abscesses should cover a broad spectrum of bacteria, including both aerobic and anaerobic organisms. Amoxicillin-clavulanate is a common choice due to its effectiveness against Gram-positive and Gram-negative bacteria. The duration of antibiotic therapy is typically determined based on the severity of the infection and the patient’s response.
Age-Dependent Imaging Modalities:
Mammography:
-
Indication and Age Cutoff: Mammography is a standard breast imaging modality, and it is the primary screening tool for breast cancer.
-
Age Cutoff: Mammography is the first-line screening tool for breast cancer in women aged 40 and older. Routine mammographic screening is vital for early detection and has been shown to reduce mortality in this age group.
-
-
Advantages:
-
Sensitivity to Microcalcifications: Mammography is particularly effective in detecting microcalcifications, which can be an early sign of breast cancer.
-
Whole-Breast Imaging: It provides a comprehensive view of the entire breast tissue.
-
-
Considerations:
-
Breast Density: Mammography may be less sensitive in women with dense breast tissue, and additional imaging modalities may be considered in such cases.
-
Ultrasound:
-
Indication and Age Cutoff: Ultrasound is often utilized as a complementary imaging tool, especially in specific clinical scenarios.
-
Age Cutoff: While there isn’t a strict age cutoff, ultrasound is commonly used alongside mammography, especially in younger women or when further lesion characterization is needed.
-
-
Advantages:
-
Soft Tissue Differentiation: Ultrasound is an excellent tool for distinguishing between fluid-filled lesions (such as cysts) and solid masses.
-
Dynamic Real-Time Imaging: It provides real-time imaging, aiding in procedures like needle aspirations and guiding interventions.
-
-
Considerations:
-
Supplemental Imaging: It is often employed as a supplemental tool in cases of dense breast tissue, screening high-risk patients, or evaluating palpable masses.
-
In some cases, surgical drainage may be necessary to evacuate purulent material and promote faster resolution. Such a fact is especially true for larger abscesses or those not responding to antibiotic therapy alone.
Preventive measures include meticulous surgical technique, perioperative antibiotic prophylaxis, and postoperative wound care. Close follow-up with the surgical team is essential to monitor for recurrence and promptly address any complications.
Case Contributed by Dr. Victor Vaz PGY2 (Mount Auburn Hospital/Harvard Medical School, Boston, MA)
References:
- Brook I. Microbiology and Management of Soft Tissue and Muscle Infections. Int J Surg. 2008;6(4):328-38.
- Lee KT, Lee MW. Cutibacterium (Propionibacterium) avidum: A Rare Pathogen Causing Breast Abscess. Cureus. 2021;13(6):e15765. doi:10.7759/cureus.15765.
- Tognetti L, Martinelli C, Berti S, et al. Cutibacterium (formerly Propionibacterium) avidum, an emerging pathogen in central nervous system shunt infection: a case report. BMC Infect Dis. 2019;19(1):350. doi:10.1186/s12879-019-3982-1.
- American College of Radiology (ACR). ACR Appropriateness Criteria®. Breast Cancer Screening. Published 2021. https://acsearch.acr.org/docs/
69427/Narrative/. - National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Breast Cancer Screening and Diagnosis. Version 3.2023.PublishedJuly2023:https
://www.nccn.org/professionals/ physician_gls/pdf/breast- screening.pdf.

Born amidst the rugged beauty of Denver, Colorado, Dr. Erin Huntley‘s journey has been defined by a commitment to compassionate healthcare. She pursued medical education at the University of North Texas and stayed in Fort Worth, for Obstetric and Gynecology residency at John Peter Smith Hospital, a county hospital known for immigrant and under-resourced populations.
Driven by a desire to serve in marginalized communities, Dr. Huntley ventured into local and Indian health in Alaska, migrant health populations in Oregon, rural Guatemalan communities, and the resource limited rural Liberia, Africa, where she practiced as a dedicated General Obstetrician and Gynecologist. Alongside her husband, a family medicine physician, she created and implemented a maternal health service line for rural Liberians that decreased maternal mortality by 85%, established a gynecology clinic, and taught lay healthcare workers point-of-care obstetric ultrasound. Her experiences in these varied settings shaped her understanding of healthcare disparities and strengthened her resolve to make a difference in the lives of women and families.
Returning to her hometown of Denver, Dr. Huntley took the opportunity to start her own family while continuing her medical career at a federally qualified health center serving refugee, underinsured, and undocumented immigrant families. However, her thirst for knowledge, her passion for advancing obstetric care, and deep interest in point-of-care ultrasound led her to pursue a fellowship in Maternal Fetal Medicine at the University of Texas Houston. Here, she honed her expertise in ultrasound and fetal anomalies, developed a keen eye for intricate details crucial in prenatal care. Additionally, as the assistant program director to the Family Medicine Obstetric Fellowship at the University of Texas at Houston, she implemented an ultrasound education program to physicians who seek careers in rural medicine.
Currently, Dr. Huntley serves as the Ultrasound Lead at Obstetrix of Colorado, where she persists in her commitment to excellence to provide the highest standard of care. Beyond her clinical duties, she remains deeply engaged in research within the field of maternal-fetal medicine, striving to enhance prenatal diagnosis and quality care for expectant mothers and engaged in mentorship for those pursuing medical careers.
Outside of her professional endeavors, Dr. Huntley finds solace and rejuvenation in the great outdoors, indulging her love for hiking, biking, and trail running. A passionate advocate for environmental sustainability, she also finds joy in teaching her daughters beekeeping and home sustainable gardening.
GUSI in the Community

GUSI was privileged to contribute to the education of physicians in the Republic of Somaliland, a region where access to healthcare resources is often limited. Leveraging our virtual POCUS platform, participants were provided with access to comprehensive online courses and quizzes aimed at imparting knowledge and skills in point-of-care ultrasound. With a federal budget of $420 million, only 6% of which is allocated to healthcare, the region faces significant challenges in delivering adequate medical services. Many hospitals lack access to advanced imaging technologies such as CTs and MRIs, making bedside PoCUS training programs invaluable in enhancing diagnostic capabilities and elevating patient care standards in resource-constrained environments.

GUSI’s very own Dr. Mena Ramos joined the panel at the Butterfly Launch Event to unveil the new iQ3. She provided insights on the use of POCUS tools that are enhancing patient care, showcasing how innovation and expertise come together to push the boundaries of what’s possible at the point of care. It’s an exciting time for GUSI and the future of ultrasound technology!

Our recent POCUS training workshop at OSU College of Osteopathic Medicine at the Cherokee Nation highlighted the pivotal role of POCUS in patient care. Given the unique challenges faced by the native population, including health disparities and travel limitations, POCUS emerges as a time-saving and convenient solution. We take pride in equipping participants with essential POCUS skills, empowering them to make a significant impact in their communities.

The OB POCUS Review course in San Francisco was a resounding success! Led by expert POCUS faculty and employing a flipped classroom approach, participants had the opportunity to scan live pregnant models. This 8-CME POCUS course left each attendee feeling enriched and empowered.

The GUSI Team participated in the 27th KAP Scientific Conference 2024 under the theme “Harnessing the power of person-centered care”. At the conference, we offered a half-day hands-on session on Focused Assessment With Sonography in Trauma (FAST) and Lung Ultrasound (LUS), empowering physicians with essential skills to provide timely care to their patients. We believe that by equipping healthcare professionals with the necessary tools and knowledge, we can further enhance person-centered care and improve patient outcomes.
Coming in March – GUSI’s scanOne™ App!

GUSI’s scanOne™ mobile app offers a fast, secure, HIPAA-compliant solution to anonymize and upload POCUS images from any ultrasound device. The scanOne app ensures accuracy and data integrity, to support sharing scans for QA and credentialing. Learn more.
“Celebrating the strength, resilience, and magic of women today and every day!”